Methicillin-resistant Staphylococcus aureus (
MRSA) is a
bacterium responsible for several difficult-to-treat
infections in humans. It is also called
oxacillin-resistant Staphylococcus aureus (
ORSA). MRSA is any strain of
Staphylococcus aureus that has developed, through the process of
natural selection,
resistance to
beta-lactam antibiotics, which include the
penicillins (
methicillin,
dicloxacillin,
nafcillin,
oxacillin, etc.) and the
cephalosporins. Strains unable to resist these antibiotics are classified as methicillin-sensitive
Staphylococcus aureus, or MSSA. The
evolution of such resistance does not cause the organism to be more intrinsically
virulent than strains of
Staphylococcus aureus
that have no antibiotic resistance, but resistance does make MRSA
infection more difficult to treat with standard types of antibiotics and
thus more dangerous.
MRSA is especially troublesome in hospitals, prisons and nursing
homes, where patients with open wounds, invasive devices, and weakened
immune systems are at greater risk of
infection than the general public.
Signs and symptoms
S. aureus most commonly colonizes the
anterior nares (the
nostrils). The rest of the
respiratory tract, open wounds,
intravenous catheters, and the
urinary tract
are also potential sites for infection. Healthy individuals may carry
MRSA asymptomatically for periods ranging from a few weeks to many
years. Patients with
compromised immune systems are at a significantly greater risk of symptomatic
secondary infection.
In most patients, MRSA can be detected by swabbing the nostrils and
isolating the bacteria found inside. Combined with extra sanitary
measures for those in contact with infected patients, screening patients
admitted to hospitals has been found to be effective in minimizing the
spread of MRSA in hospitals in the United States,
[1] Denmark,
Finland, and the
Netherlands.
[2]
MRSA may progress substantially within 24–48 hours of initial topical
symptoms. After 72 hours, MRSA can take hold in human tissues and
eventually become resistant to treatment.
The initial presentation of
MRSA is small red bumps that resemble pimples, spider bites, or boils;
they may be accompanied by fever and, occasionally, rashes. Within a few
days, the bumps become larger and more painful; they eventually open
into deep, pus-filled boils.[3]
About 75 percent of community-associated (CA-) MRSA infections are
localized to skin and soft tissue and usually can be treated
effectively.[4] But some CA-MRSA strains display enhanced virulence,
spreading more rapidly and causing illness much more severe than
traditional healthcare-associated (HA-) MRSA infections, and they can
affect vital organs and lead to widespread infection (sepsis), toxic shock syndrome, and necrotizing ("flesh-eating") pneumonia. This is thought to be due to toxins carried by CA-MRSA strains, such as PVL and PSM, though PVL was recently found not to be a factor in a study by the National Institute of Allergy and Infectious Diseases (NIAID) at the National Institutes of Health. (
NIH)
It is not known why some healthy people develop CA-MRSA skin infections
that are treatable while others infected with the same strain develop
severe infections or die.
[5]
People are very commonly colonized with CA-MRSA and are completely
asymptomatic. The most common manifestations of CA-MRSA are simple skin
infections, such as
impetigo,
boils,
abscesses,
folliculitis, and
cellulitis. Rarer, but more serious manifestations can occur, such as
necrotizing fasciitis and
pyomyositis (most commonly found in the tropics),
necrotizing pneumonia,
infective endocarditis (which affects the valves of the heart), and bone and joint infections.
[6]
CA-MRSA often results in abscess formation that requires incision and
drainage. Before the spread of MRSA into the community, abscesses were
not considered contagious, because it was assumed that infection
required violation of skin integrity and the introduction of
staphylococci from normal skin colonization. However, newly emerging
CA-MRSA is transmissible (similar, but with very important differences)
from Hospital-Associated MRSA. CA-MRSA is less likely than other forms
of MRSA to cause
cellulitis.
Risk factors
Some of the populations at risk:
- People with weak immune systems (HIV/AIDS, lupus, or cancer sufferers; transplant recipients, severe asthmatics, etc.)
- Diabetics[7] *
- Intravenous drug users [8]
- Users of quinolone antibiotics[9]
- Young children[citation needed]
- The elderly[citation needed]8
- College students living in dormitories[8]
- People staying or working in a health care facility for an extended period of time[8]
- People who spend time in coastal waters where MRSA is present, such as some beaches in Florida and the west coast of the United States[10][11]
- People who spend time in confined spaces with other people, including occupants of homeless shelters and warming centers, prison inmates, military recruits in basic training,[12] and individuals who spend considerable time in changerooms or gyms.[citation needed]
- Veterinarians, livestock handlers, and pet owners[13]
Hospital patients
Many MRSA infections occur in hospitals and healthcare facilities.
When infections occur in this manner it is known as healthcare acquired
MRSA or HA-MRSA. These Rates of MRSA infection are also increased in
hospitalized patients who are treated with
quinolones.
Healthcare provider-to-patient transfer is common, especially when
healthcare providers move from patient to patient without performing
necessary hand-washing techniques between patients.
[9][14]
Prison inmates, military recruits, and the homeless
Prisons, military barracks, and homeless shelters can be crowded and
confined, and poor hygiene practices may proliferate, thus putting
inhabitants at increased risk of contracting MRSA.
[13]
Cases of MRSA in such populations were first reported in the United
States, and then in Canada. The earliest reports were made by the
Center for Disease Control
(CDC) in US state prisons. Subsequently reports of a massive rise in
skin and soft tissue infections were reported by the CDC in the
Los Angeles
County Jail system in 2001, and this has continued. Pan et al. reported
on the changing epidemiology of MRSA skin infection in the
San Francisco
County Jail, noting MRSA accounted for more than 70% of S. aureus
infection in the jail by 2002. Lowy and colleagues reported on frequent
MRSA skin infections in
New York State Prisons. Two reports on inmates in Maryland have demonstrated frequent colonization with MRSA.
In the news media hundreds of reports of MRSA outbreaks in prisons
appeared between 2000 and 2008. For example, in February 2008, the
Tulsa County Jail in the U.S. State of
Oklahoma started treating an average of twelve Staphylococcus cases per month.
[15] A report on skin and soft tissue infections in the
Cook County Jail in
Chicago
in 2004–05 demonstrated that MRSA was the most common cause of these
infections among cultured lesions and furthermore that few risk factors
were more strongly associated with MRSA infections than infections
caused by methicillin-susceptible S. aureus. In response to these and
many other reports on MRSA infections among incarcerated and recently
incarcerated persons, the
Federal Bureau of Prisons
has released guidelines for the management and control of the
infections although few studies provide an evidence base for these
guidelines.
People in contact with live food-producing animals
Cases of MRSA have increased in livestock animals. CC398 is a new
variant of MRSA that has emerged in animals and is found in intensively
reared production animals (primarily pigs, but also cattle and poultry),
where it can be transmitted to humans. Though dangerous to humans,
CC398 is often asymptomatic in food-producing animals.
[16]
A 2011 study reported 47% of the meat and poultry sold in surveyed
U.S. grocery stores was contaminated with S. aureus and, of those,
52%—or 24.4% of the total—were resistant to at least three classes of
antibiotics. "Now we need to determine what this means in terms of risk
to the consumer," said Dr. Keim, a co-author of the paper.
[17] Some samples of commercially sold meat products in Japan were also found to harbor MRSA strains.
[18]
Athletes
In the United States, there have been increasing numbers of reports
of outbreaks of MRSA colonization and infection through skin contact in
locker rooms and
gyms, even among healthy populations.
[citation needed] A study published in the
New England Journal of Medicine linked MRSA to the abrasions caused by artificial turf.
[19]
Three studies by the Texas State Department of Health found that the
infection rate among football players was 16 times the national average.
In October 2006, a high school football player was temporarily
paralyzed from MRSA-infected turf burns. His infection returned in
January 2007 and required three surgeries to remove infected tissue, as
well as three weeks of hospital stay.
[20] In 2013,
Lawrence Tynes,
Carl Nicks, and
Johnthan Banks of the
Tampa Bay Buccaneers
were diagnosed with MRSA. Tynes and Nicks are not believed to have
contracted the infection from each other, but it is unknown if Banks
contracted it from either individual.
[21]
Children
MRSA is also becoming a problem in pediatric settings,
[22] including hospital nurseries.
[23] A 2007 study found that 4.6% of patients in U.S. health care facilities were infected or colonized with MRSA.
[24]
MRSA is becoming a major health concern in children because they are
more likely to exhibit minor scrapes, cuts, bruises, and bug bites than
adults. Children as well as adults are at higher risk of getting MRSA
who come in contact with day care centers, playgrounds, locker rooms,
camps, dormitories, classrooms and other school settings, and gyms and
workout facilities. Parents should be especially cautious of children
who participate in activities where there is shared sports equipment
such as football helmets and uniforms.
[25]
Diagnosis
Diagnostic microbiology laboratories and reference laboratories are
key for identifying outbreaks of MRSA. New rapid techniques for the
identification and characterization of MRSA have been developed.
[26] This notwithstanding, the bacterium generally must be cultured via blood, urine,
sputum,
or other body fluid cultures, and cultured in the lab in sufficient
quantities to perform these confirmatory tests first. Consequently,
there is no quick and easy method to diagnose a MRSA infection.
Therefore, initial treatment is often based upon 'strong suspicion' by
the treating physician, since any delay in treating this type of
infection can have fatal consequences. These techniques include
quantitative PCR and are increasingly being employed in clinical laboratories for the rapid detection and identification of MRSA strains.
[27][28]
Another common laboratory test is a rapid
latex agglutination test that detects the PBP2a protein. PBP2a is a variant
penicillin-binding protein that imparts the ability of S. aureus to be resistant to oxacillin.
[29]
Genetics
Antimicrobial resistance is genetically based; resistance is mediated
by the acquisition of extrachromosomal genetic elements containing
resistance genes. Exemplary are plasmids, transposable genetic elements,
and genomic islands, which are transferred between bacteria via
horizontal gene transfer.
[30] A defining characteristic of MRSA is its ability to thrive in the presence of
penicillin-like antibiotics, which normally prevent bacterial growth by inhibiting synthesis of
cell wall material. This is due to a resistance gene,
mecA, which stops β-lactam antibiotics from inactivating the enzymes (transpeptidases) that are critical for cell wall synthesis.
SCCmec
Staphylococcal
cassette chromosome mec (
SCCmec) is a genomic island of unknown origin containing the antibiotic resistance gene
mecA.
[31][32] SCC
mec contains additional genes beyond
mecA, including the
cytolysin gene
psm-mec, which may suppress virulence in hospital-acquired MRSA strains.
[33] SCC
mec also contains
ccrA and
ccrB; both genes encode recombinases that mediate the site-specific integration and excision of the SCC
mec element from the
S. aureus chromosome.
[31][32] Currently, six unique SCC
mec types ranging in size from 21–67 kb have been identified;
[31] they are designated types I-VI and are distinguished by variation in
mec and
ccr gene complexes.
[30] Owing to the size of the SCC
mec
element and the constraints of horizontal gene transfer, a limited
number of clones is thought to be responsible for the spread of MRSA
infections.
[31]
Different SCC
mec genotypes confer different microbiological characteristics, such as different antimicrobial resistance rates.
[34] Different genotypes are also associated with different types of infections. Types I-III SCC
mec are large elements that typically contain additional resistance genes and are characteristically isolated from HA-MRSA strains.
[32][34] Conversely, CA-MRSA is associated with types IV and V, which are smaller and lack resistance genes other than
mecA.
[32][34]
mecA
mecA is responsible for resistance to methicillin and other β-lactam antibiotics. After acquisition of
mecA, the gene must be integrated and localized in the S. aureus chromosome.
[31] mecA
encodes penicillin-binding protein 2a (PBP2a), which differs from other
penicillin-binding proteins as its active site does not bind
methicillin or other β-lactam antibiotics.
[31] As such, PBP2a can continue to catalyze the transpeptidation reaction required for
peptidoglycan
cross-linking, enabling cell wall synthesis in the presence of
antibiotics. As a consequence of the inability of PBP2a to interact with
β-lactam moieties, acquisition of
mecA confers resistance to all β-lactam antibiotics in addition to methicillin.
[31][35]
mecA is under the control of two
regulatory genes,
mecI and
mecR1. MecI is usually bound to the
mecA promoter and functions as a repressor.
[30][32] In the presence of a β-lactam antibiotic, MecR1 initiates a
signal transduction cascade that leads to transcriptional activation of
mecA.
[30][32] This is achieved by MecR1-mediated cleavage of MecI, which alleviates MecI repression.
[30] mecA is further controlled by two co-repressors, BlaI and BlaR1.
blaI and
blaR1 are homologous to
mecI and
mecR1, respectively, and normally function as regulators of
blaZ, which is responsible for penicillin resistance.
[31][36] The DNA sequences bound by MecI and BlaI are identical;
[31] therefore, BlaI can also bind the
mecA operator to repress transcription of
mecA.
[36]
Strains
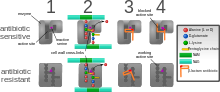
Diagram depicting antibiotic resistance through alteration of the
antibiotic's target site, modeled after MRSA's resistance to penicillin.
Beta-lactam antibiotics permanently inactivate
PBP enzymes,
which are essential for bacterial life, by permanently binding to their
active sites. Some forms of MRSA, however, express a PBP that will not
allow the antibiotic into their active site.
Acquisition of SCC
mec in methicillin-sensitive staphylococcus aureus (
MSSA)
gives rise to a number of genetically different MRSA lineages. These
genetic variations within different MRSA strains possibly explain the
variability in virulence and associated MRSA infections.
[37] The first MRSA strain, ST250 MRSA-1 originated from SCC
mec and ST250-MSSA integration.
[37]
Historically, major MRSA clones: ST2470-MRSA-I, ST239-MRSA-III,
ST5-MRSA-II, and ST5-MRSA-IV were responsible for causing
hospital-acquired MRSA (HA-MRSA) infections.
[37]
ST239-MRSA-III, known as the Brazilian clone, was highly transmissible
compared to others and distributed in Argentina, Czech Republic, and
Portugal.
[37]
In the UK, where MRSA is commonly called "Golden Staph", the most common strains of MRSA are EMRSA15 and EMRSA16.
[38] EMRSA16 is the best described epidemiologically: it originated in
Kettering, England, and the full genomic sequence of this strain has been published.
[39] EMRSA16 has been found to be identical to the
ST36:USA200 strain, which circulates in the United States, and to carry the SCC
mec type II,
enterotoxin A and
toxic shock syndrome toxin 1 genes.
[40]
Under the new international typing system, this strain is now called
MRSA252. EMRSA 15 is also found to be one of the common MRSA strains in
Asia. Other common strains include ST5:USA100 and EMRSA 1.
[41] These strains are genetic characteristics of HA-MRSA.
[42]
It is not entirely certain why some strains are highly transmissible and persistent in healthcare facilities.
[37]
One explanation is the characteristic pattern of antibiotic
susceptibility. Both the EMRSA15 and EMRSA16 strains are resistant to
erythromycin and
ciprofloxacin. It is known that
Staphylococcus aureus can survive intracellularly,
[43] for example in the nasal mucosa
[44] and in the tonsil tissue.
[45]
Erythromycin and Ciprofloxacin are precisely the antibiotics that best
penetrate intracellularly; it may be that these strains of
S. aureus are therefore able to exploit an intracellular niche.
Community-acquired MRSA (CA-MRSA) strains emerged in late 1990 to
2000, infecting healthy people who had not been in contact with health
care facilities.
[42]
A later study that analyzed data from more than 300 microbiology labs
associated with hospitals all over the United States have found a
seven-fold increase, jumping from 3.6% of all MRSA infections to 28.2%,
in the proportion of community-associated strains of MRSA between 1999
and 2006.
[46] Researchers suggest that CA-MRSA did not evolve from the HA-MRSA.
[42] This is further proven by molecular typing of CA-MRSA strains
[47] and genome comparison between CA-MRSA and HA-MRSA, which indicate that novel MRSA strains integrated SCC
mec into MSSA separately on its own.
[42]
By mid 2000, CA-MRSA was introduced into the health care systems and
distinguishing CA-MRSA from HA-MRSA became a difficult process.
[42] Community-acquired MRSA (CA-MRSA) is more easily treated and more virulent than hospital-acquired MRSA (HA-MRSA).
[42] The genetic mechanism for the enhanced virulence in CA-MRSA remains an active area of research. Especially the
Panton-Valentine leukocidin (PVL) genes are of interest because they are a unique feature of CA-MRSA.
[37]
In the United States, most cases of CA-MRSA are caused by a CC8 strain designated
ST8:USA300, which carries SCC
mec type IV,
Panton-Valentine leukocidin,
PSM-alpha and
enterotoxins Q and K,
[40] and
ST1:USA400.
[48]
The ST8:USA300 strain results in skin infections, necrotizing fasciitis
and toxic shock syndrome, whereas the ST1:USA400 strain results in
necrotizing pneumonia and pulmonary sepsis.
[37]
Other community-acquired strains of MRSA are ST8:USA500 and
ST59:USA1000. In many nations of the world, MRSA strains with different
predominant genetic background types have come to predominate among
CA-MRSA strains; USA300 easily tops the list in the U. S. and is
becoming more common in Canada after its first appearance there in 2004.
For example, in Australia ST93 strains are common, while in continental
Europe ST80 strains (Tristan et al., Emerging Infectious Diseases,
2006), which carry SCC
mec type IV, predominate.
[49]
In Taiwan, ST59 strains, some of which are resistant to many
non-beta-lactam antibiotics, have arisen as common causes of skin and
soft tissue infections in the community. In a remote region of Alaska,
unlike most of the continental U. S., USA300 was found rarely in a study
of MRSA strains from outbreaks in 1996 and 2000 as well as in
surveillance from 2004–06 (David et al., Emerg Infect Dis 2008).
In June 2011, the discovery of a new strain of MRSA was announced by
two separate teams of researchers in the UK. Its genetic makeup was
reportedly more similar to strains found in animals, and testing kits
designed to detect MRSA were unable to identify it.
[50] This MRSA strain,
Clonal Complex 398 (CC398), is responsible for Livestock-associated MRSA (LA-MRSA) infections.
[41] Although it is known to be more persistent in colonizing pigs and calves, there have been cases of LA-MRSA carriers with
pneumonia,
endocarditis, and
necrotising fasciitis.
[51]
Prevention
Screening programs
Patient screening upon hospital admission, with nasal cultures,
prevents the cohabitation of MRSA carriers with non-carriers, and
exposure to infected surfaces. The test used (whether a rapid molecular
method or traditional culture) is not as important as the implementation
of active screening.
[52]
In the United States and Canada, the Centers for Disease Control and
Prevention issued guidelines on October 19, 2006, citing the need for
additional research, but declined to recommend such screening.
[53][54]
In some UK hospitals screening for MRSA is performed in every patient
[55] and all NHS surgical patients, except for minor surgeries, are previously checked for MRSA.
[56] There is no community screening in the UK; however, screening of individuals is offered by some private companies.
[57]
In a US cohort of 1300 healthy children, 2.4% carried MRSA in their nose.
[58]
Surface sanitizing

NAV-CO2 sanitizing in Pennsylvania hospital exam room
Alcohol has been proven to be an effective surface sanitizer against MRSA.
Quaternary ammonium can be used in conjunction with alcohol to extend the longevity of the sanitizing action.
[citation needed] The prevention of
nosocomial infections involves routine and
terminal cleaning.
Non-flammable Alcohol Vapor in Carbon Dioxide systems (NAV-CO2) do not corrode metals or plastics used in medical environments and do not contribute to antibacterial resistance.
In healthcare environments, MRSA can survive on surfaces and fabrics,
including privacy curtains or garments worn by care providers. Complete
surface sanitation is necessary to eliminate MRSA in areas where
patients are recovering from invasive procedures. Testing patients for
MRSA upon admission, isolating MRSA-positive patients, decolonization of
MRSA-positive patients, and
terminal cleaning of patients' rooms and all other clinical areas they occupy is the current best practice protocol for nosocomial MRSA.
Studies published from 2004-2007 reported hydrogen peroxide vapor
could be used to decontaminate busy hospital rooms, despite taking
significantly longer than traditional cleaning. One study noted rapid
recontamination by MRSA following the hydrogen peroxide application.
[59][60][61][62][63]
Also tested, in 2006, was a new type of surface cleaner,
incorporating accelerated hydrogen peroxide, which was pronounced "a
potential candidate" for use against the targeted microorganisms.
[64]
Research on copper alloys
In 2008, after evaluating a wide body of research mandated specifically by the
United States Environmental Protection Agency
(EPA), registration approvals were granted by EPA in 2008 granting that
copper alloys kill more than 99.9% of MRSA within two hours.
Subsequent research conducted at the University of Southampton (UK)
compared the antimicrobial efficacies of copper and several non-copper
proprietary coating products to kill MRSA.
[65][66]
At 20 °C, the drop-off in MRSA organisms on copper alloy C11000 is
dramatic and almost complete (over 99.9% kill rate) within 75 minutes.
However, neither a triclosan-based product nor two silver-containing
based antimicrobial treatments (Ag-A and Ag-B) exhibited any meaningful
efficacy against MRSA. Stainless steel S30400 did not exhibit any
antimicrobial efficacy.
In 2004, the University of Southampton research team was the first to clearly demonstrate that copper inhibits MRSA.
[67]
On copper alloys — C19700 (99% copper), C24000 (80% copper), and C77000
(55% copper) — significant reductions in viability were achieved at
room temperatures after 1.5 hours, 3.0 hours and 4.5 hours,
respectively. Faster antimicrobial efficacies were associated with
higher copper alloy content. Stainless steel did not exhibit any
bactericidal benefits.
Hand washing
In September 2004,
[68] after a successful pilot scheme to tackle MRSA, the UK
National Health Service announced its
Clean Your Hands campaign. Wards were required to ensure that
alcohol-based hand rubs
are placed near all beds so that staff can hand wash more regularly. It
is thought that even if this cuts infection by no more than 1%, the
plan will pay for itself many times over.
[citation needed]
As with some other bacteria, MRSA is acquiring more resistance to some
disinfectants and
antiseptics.
Although alcohol-based rubs remain somewhat effective, a more effective
strategy is to wash hands with running water and an anti-microbial
cleanser with persistent killing action, such as
Chlorhexidine.
[69] In another study
chlorohexidine (Hibiclens),
p-chloro-
m-xylenol (Acute-Kare),
hexachlorophene (Phisohex), and
povidone-iodine
(Betadine) were evaluated for their effectiveness. Of the four most
commonly used antiseptics, povidone-iodine, when diluted 1:100, was the
most rapidly bactericidal against both MRSA and methicillin-susceptible
S.
aureus.
[70]
A June 2008 report, centered on a survey by the Association for
Professionals in Infection Control and Epidemiology, concluded that poor
hygiene habits remain the principal barrier to significant reductions
in the spread of MRSA.
Proper disposal of hospital gowns
Used paper
hospital gowns are associated with MRSA hospital infections, which could be avoided by proper disposal.
[71]
Isolation
Excluding
medical facilities, current US guidance does not require workers with MRSA infections to be routinely excluded from the general workplace.
[72]
Therefore, unless directed by a health care provider, exclusion from
work should be reserved for those with wound drainage that cannot be
covered and contained with a clean, dry bandage and for those who cannot
maintain good hygiene practices.
[72]
Workers with active infections should be excluded from activities where
skin-to-skin contact is likely to occur until their infections are
healed. Health care workers should follow the Centers for Disease
Control and Prevention's Guidelines for Infection Control in Health Care
Personnel.
[73]
To prevent the spread of staph or MRSA in the workplace, employers
should ensure the availability of adequate facilities and supplies that
encourage workers to practice good hygiene; that surface sanitizing in
the workplace is followed; and that contaminated equipment are sanitized
with Environmental Protection Agency (EPA)-registered disinfectants.
[72]
Restricting antibiotic use
Glycopeptides,
cephalosporins and in particular
quinolones
are associated with an increased risk of colonisation of MRSA. Reducing
use of antibiotic classes that promote MRSA colonisation, especially
fluoroquinolones, is recommended in current guidelines.
[9][14]
Public health considerations
Mathematical models describe one way in which a loss of infection
control can occur after measures for screening and isolation seem to be
effective for years, as happened in the UK. In the "search and destroy"
strategy that was employed by all UK hospitals until the mid-1990s, all
patients with MRSA were immediately isolated, and all staff were
screened for MRSA and were prevented from working until they had
completed a course of eradication therapy that was proven to work. Loss
of control occurs because colonised patients are discharged back into
the community and then readmitted; when the number of colonised patients
in the community reaches a certain threshold, the "search and destroy"
strategy is overwhelmed.
[74] One of the few countries not to have been overwhelmed by MRSA is the
Netherlands:
An important part of the success of the Dutch strategy may have been to
attempt eradication of carriage upon discharge from hospital.
[75]
The Centers for Disease Control and Prevention (CDC) estimated that
about 1.7 million nosocomial infections occurred in the United States in
2002, with 99,000 associated deaths.
[76]
The estimated incidence is 4.5 nosocomial infections per 100
admissions, with direct costs (at 2004 prices) ranging from $10,500
(£5300, €8000 at 2006 rates) per case (for bloodstream, urinary tract,
or respiratory infections in immunocompetent patients) to $111,000
(£57,000, €85,000) per case for antibiotic-resistant infections in the
bloodstream in patients with transplants. With these numbers,
conservative estimates of the total direct costs of nosocomial
infections are above $17 billion. The reduction of such infections forms
an important component of efforts to improve healthcare safety. (BMJ
2007)
[citation needed]
MRSA alone was associated with 8% of nosocomial infections reported to
the CDC National Healthcare Safety Network from January 2006 to October
2007.
[77]
This problem is not unique to one country; the British National Audit
Office estimated that the incidence of nosocomial infections in Europe
ranges from 4% to 10% of all hospital admissions. As of early 2005, the
number of deaths in the United Kingdom attributed to MRSA has been
estimated by various sources to lie in the area of 3,000 per year.
[78] Staphylococcus
bacteria account for almost half of all UK hospital infections. The
issue of MRSA infections in hospitals has recently been a major
political issue in the UK, playing a significant role in the debates
over health policy in the
United Kingdom general election held in 2005.
On January 6, 2008, half of 64 non-Chinese cases of MRSA infections in
Hong Kong in 2007 were
Filipino domestic helpers. Ho Pak-leung, professor of microbiology at the
University of Hong Kong,
traced the cause to high use of antibiotics. In 2007, there were 166
community cases in Hong Kong compared with 8,000 hospital-acquired MRSA
cases (155 recorded cases—91 involved Chinese locals, 33 Filipinos, 5
each for Americans and Indians, and 2 each from Nepal, Australia,
Denmark and England).
[79]
Worldwide, an estimated 2 billion people carry some form of
S. aureus; of these, up to 53 million (2.7% of carriers) are thought to carry MRSA.
[80] In the United States, 95 million carry
S. aureus in their noses; of these, 2.5 million (2.6% of carriers) carry MRSA.
[81]
A population review conducted in three U.S. communities showed the
annual incidence of CA-MRSA during 2001–2002 to be 18–25.7/100,000; most
CA-MRSA isolates were associated with clinically relevant infections,
and 23% of patients required hospitalization.
[82]
One possible contribution to the increased spread of MRSA infections comes from the use of antibiotics in
intensive pig farming.
A 2008 study in Canada found MRSA in 10% of tested pork chops and
ground pork; a U.S. study in the same year found MRSA in the noses of
70% of the tested farm pigs and in 45% of the tested pig farm workers.
[83] There have also been anecdotal reports of increased MRSA infection rates in rural communities with pig farms.
[84]
Healthcare facilities with high bed occupancy rates, high levels of
temporary nursing staff, or low cleanliness scores no longer have
significantly higher MRSA rates. Simple tabular evidence helps provide a
clear picture of these changes, showing, for instance, that hospitals
with occupancy over 90% had, in 2006–2007, MRSA rates little above those
in hospitals with occupancy below 85%, in contrast to the period
2001–2004. In one sense, the disappearance of these relationships is
puzzling. Reporters now blame IV cannula and catheters for spreading
MRSA in hospitals. (Hospital organisation and speciality mix, 2008)
[citation needed]
Decolonization
Care should be taken when trying to drain boils, as disruption of
surrounding tissue can lead to larger infections, or even infection of
the blood stream (often with fatal consequences).
[85]
Any drainage should be disposed of very carefully. After the drainage
of boils or other treatment for MRSA, patients can shower at home using
chlorhexidine (Hibiclens) or
hexachlorophene
(Phisohex) antiseptic soap (available over-the-counter at many
pharmacies) from head to toe. Alternatively, a dilute bleach bath can be
taken at a concentration of 2.5 μL/mL dilution of bleach (about 1/2 cup
bleach per 1/4-full bathtub of water).
[86] Care should be taken to use a clean towel, and to ensure that nasal discharge doesn't infect the towel (see below).
All infectious lesions should be kept covered with a dressing.
[85] Mupirocin (Bactroban) 2% ointment can be effective at reducing the size of lesions. A secondary covering of clothing is preferred.
[87]
As shown in an animal study with diabetic mice, the topical application
of a mixture of sugar (70%) and 3% povidone-iodine paste is an
effective agent for the treatment of diabetic ulcers with MRSA
infection.
[88]
The nose is a common refuge for MRSA, and a test swab can be taken of the nose to indicate whether MRSA is present.
[89] If MRSA is detected via nasal culture,
Mupirocin
(Bactroban) 2% ointment can be applied inside each nostril twice daily
for 7 days, using a cotton-tipped swab. However, care should be taken so
that the swab doesn't penetrate into the sinus. Household members are
recommended to follow the same decolonization protocol. After treatment,
the nose should be swabbed again to ensure that the treatment was
effective. If not, the process should be repeated.
Toilet seats are a common vector for infection, and wiping seats
clean before and/or after use can help to prevent the spread of MRSA.
Door handles, faucets, light switches (with care!), etc. can be
disinfected regularly with disinfectant wipes.
[87]
Spray disinfectants can be used on upholstery. Carpets can be washed
with disinfectant, and hardwood floors can be scrubbed with diluted tea
tree oil (e.g. Melaleuca). Laundry soap containing tea tree oil may be
effective at decontaminating clothing and bedding, especially if hot
water and heavy soil cycles are used, however tea tree oil may cause a
rash which MRSA can re-colonize. Alcohol-based sanitizers can be placed
near bedsides, near sitting areas, in vehicles etc. to encourage their
use.
Doctors may also prescribe antibiotics such as
clindamycin,
doxycycline or
trimethoprim/sulfamethoxazole.
The CDC offers suggestions for preventing the contraction and spread
MRSA infection which are applicable to those in community settings,
including incarcerated populations, childcare center employees, and
athletes. To prevent MRSA infection, individuals should regularly wash
hands using soap and water or an alcohol-based sanitizer, keep wounds
clean and covered, avoid contact with other people's wounds, avoid
sharing personal items such as razors or towels, shower after exercising
at athletic facilities (including gyms, weight rooms, and school
facilities), shower before using swimming pools or whirlpools, and
maintain a clean environment.
[90]
It may be difficult for people to maintain the necessary cleanliness
if they do not have access to facilities such as public toilets with
handwashing facilities. In the United Kingdom, the
Workplace (Health, Safety and Welfare) Regulations 1992
requires businesses to provide toilets for their employees, along with
washing facilities including soap or other suitable means of cleaning.
Guidance on how many toilets to provide and what sort of washing
facilities should be provided alongside them is given in the Workplace
(Health, Safety and Welfare) Approved Code of Practice and Guidance L24,
available from
Health and Safety Executive Books. But there is no legal obligation on local authorities in the United Kingdom to provide
public toilets,
and although in 2008 the House of Commons Communities and Local
Government Committee called for a duty on local authorities to develop a
public toilet strategy
[1] this was rejected by the Government
[2].
Treatment
Both CA-MRSA and HA-MRSA are resistant to traditional anti-staphylococcal
beta-lactam antibiotics, such as
cephalexin. CA-MRSA has a greater spectrum of antimicrobial susceptibility, including to
sulfa drugs (like
co-trimoxazole/trimethoprim-sulfamethoxazole),
tetracyclines (like
doxycycline and
minocycline) and
clindamycin (for
osteomyelitis), but the drug of choice for treating CA-MRSA is now believed to be
vancomycin,
according to a Henry Ford Hospital Study. HA-MRSA is resistant even to
these antibiotics and often is susceptible only to vancomycin. Newer
drugs, such as
linezolid (belonging to the newer
oxazolidinones class) and
daptomycin,
are effective against both CA-MRSA and HA-MRSA. Linezolid is now felt
to be the best drug for treating patients with MRSA pneumonia.
[91][dubious – discuss]
Ceftaroline and ceftabiparole, new fifth generation cephalosporins, are
the first beta-lactam antibiotics approved in the US to treat MRSA
infections (skin and soft tissue only).
[citation needed]
Vancomycin and
teicoplanin are
glycopeptide antibiotics used to treat MRSA infections.
[92] Teicoplanin is a structural
congener of vancomycin that has a similar activity spectrum but a longer
half-life.
[93] Because the oral absorption of vancomycin and
teicoplanin is very low, these agents must be administered intravenously to control systemic infections.
[94]
Treatment of MRSA infection with vancomycin can be complicated, due to
its inconvenient route of administration. Moreover, many clinicians
believe that the efficacy of vancomycin against MRSA is inferior to that
of anti-staphylococcal
beta-lactam antibiotics against methicillin-susceptible
Staphylococcus aureus (MSSA).
[95][96]
Several newly discovered strains of MRSA show
antibiotic resistance even to vancomycin and
teicoplanin. These new evolutions of the MRSA bacterium have been dubbed
Vancomycin intermediate-resistant Staphylococcus aureus (VISA).
[97] [98] Linezolid,
quinupristin/dalfopristin,
daptomycin,
ceftaroline, and
tigecycline are used to treat more severe infections that do not respond to glycopeptides such as vancomycin.
[99] Current guidelines recommend
daptomycin for VISA bloodstream infections and endocarditis.
[100]
There have been claims that
bacteriophage can be used to cure MRSA.
[101][102]
The psychedelic mushroom
Psilocybe semilanceata has been shown to strongly inhibit the growth of
Staphylococcus aureus.
[103] The
cannabinoids CBD and
CBG powerfully inhibit MRSA,
[104] in addition to the terpenoid
pinene which occurs in
cannabis.
[105]
Initial studies at the University of East London have demonstrated that
allicin
(a compound found in garlic) exhibits a strong antimicrobial response
to the bacteria, indicating that it may one day lead to more effective
treatments.
[106]
A report released in 2010 details the efficacy of the active
ingredients of a new composite dressing (hydrogen peroxide, tobramycin,
chlorhexidine digluconate, chlorhexidine gluconate, levofloxacin, and
silver) against MRSA.
[107]
A 1990 study tested MRSA isolates obtained from veterans and found
they could be killed by several substances, including bacitracin,
nitrofurantoin, hydrogen peroxide, novobiocin, netilmicin and
vancomycin. The study went on to conclude that netilmicin might be
useful as an alternative to intravenous vancomycin, and suggested that
topical applications of hydrogen peroxide may be useful to reduce MRSA
on skin and some mucous membranes.
[108]
History
US and UK

Incidence of MRSA in human blood samples in countries which took part in the study in 2008
In 1959
methicillin was licensed in England to treat penicillin-resistant
S. aureus infections. Just as bacterial evolution had allowed microbes to develop resistance to penicillin, strains of
S. aureus
evolved to become resistant to methicillin. In 1961 the first known
MRSA isolates were reported in a British study, and between 1961-1967
there were infrequent hospital outbreaks in Western Europe and
Australia.
[109]
The first United States hospital outbreak of MRSA occurred at the
Boston City Hospital in 1968. Between 1968-mid-1990s the percent of
S. aureus
infections that were caused by MRSA increased steadily, and MRSA became
recognized as an endemic pathogen. In 1974 2% of hospital-acquired
S. aureus infections could be attributed to MRSA.
[110] The rate had increased to 22% by 1995, and by 1997 the percent of hospital
S. aureus infections attributable to MRSA had reached 50%.
The first report of CA-MRSA occurred in 1981, and in 1982 there was a
large outbreak of CA-MRSA among intravenous drug users in Detroit,
Michigan.
[109]
Additional outbreaks of CA-MRSA were reported through the 1980s and
1990s, including outbreaks among Australian Aboriginal populations that
had never been exposed to hospitals. In the mid-1990s there were
scattered reports of CA-MRSA outbreaks among US children. While HA-MRSA
rates stabilized between 1998–2008, CA-MRSA rates continued to rise. A
report released by the University of Chicago Children's Hospital
comparing two time periods (1993–1995 and 1995–1997) found a 25-fold
increase in the rate of hospitalizations due to MRSA among children in
the United States.
[111]
In 1999 the University of Chicago reported the first deaths from
invasive MRSA among otherwise healthy children in the United States.
[109] By 2004 MRSA accounted for 64% of hospital-acquired
S. aureus infections in the United States.
The
Office for National Statistics reported 1,629 MRSA-related deaths in England and Wales during 2005, indicating a MRSA-related
mortality rate
half the rate of that in the United States for 2005, even though the
figures from the British source were explained to be high because of
"improved levels of reporting, possibly brought about by the continued
high public profile of the disease"
[112] during the time of the
2005 United Kingdom General Election. MRSA is thought to have caused 1,652 deaths in 2006 in UK up from 51 in 1993.
[113]
It has been argued that the observed increased mortality among
MRSA-infected patients may be the result of the increased underlying
morbidity
of these patients. Several studies, however, including one by Blot and
colleagues, that have adjusted for underlying disease still found MRSA
bacteremia to have a higher attributable mortality than
methicillin-susceptible
S. aureus (MSSA) bacteremia.
[114]
A population-based study of the incidence of MRSA infections in
San Francisco
during 2004–05 demonstrated that nearly 1 in 300 residents suffered
from such an infection in the course of a year and that greater than 85%
of these infections occurred outside of the healthcare setting.
[115] A 2004 study showed that patients in the United States with
S. aureus
infection had, on average, three times the length of hospital stay
(14.3 vs. 4.5 days), incurred three times the total cost ($48,824 vs
$14,141), and experienced five times the risk of in-hospital death
(11.2% vs 2.3%) than patients without this infection.
[116] In a meta-analysis of 31 studies, Cosgrove
et al.,
[117]
concluded that MRSA bacteremia is associated with increased mortality
as compared with MSSA bacteremia (odds ratio = 1.93; 95% CI =
1.93±0.39).
[118] In addition, Wyllie
et al.
report a death rate of 34% within 30 days among patients infected with
MRSA, a rate similar to the death rate of 27% seen among MSSA-infected
patients.
[119]
According to the CDC, the most recent estimates of the incidence of
healthcare-associated infections that are attributable to MRSA in the
United States indicate a decline in such infection rates. Incidence of
MRSA central line-associated blood stream infections as reported by
hundreds of intensive care units decreased 50-70% from 2001-2007.
[110] A separate system tracking all hospital MRSA bloodstream infections found an overall 34% decrease between 2005-2008.
[110]
MRSA is sometimes sub-categorised as community-acquired MRSA
(CA-MRSA) or healthcare-associated MRSA (HA-MRSA), although the
distinction is complex. Some researchers have defined CA-MRSA by the
characteristics of patients whom it infects, while others define it by
the
genetic
characteristics of the bacteria themselves. By 2005, identified CA-MRSA
risk factors included athletes, military recruits, incarcerated people,
emergency room patients, urban children, HIV-positive individuals, men
who have sex with men, and indigenous populations.
[109]
Worldwide
The first reported cases of CA-MRSA began to appear in the mid-1990s
in Australia, New Zealand, the United States, the United Kingdom,
France, Finland, Canada and Samoa, and were notable because they
involved people who had not been exposed to a healthcare setting.
[6]
Because measurement and reporting varies, it is difficult to compare
rates of MRSA in different countries. An international comparison of
2004 MRSA-attributable
S. aureus rates in middle and high income
countries released by the Center For Disease Dynamics, Economics, and
Policy in showed that Iceland had the lowest rate of infection, and
Romania had the highest at over 70%.
[120]
Research
Clinical
It has been reported that
maggot therapy
to clean out necrotic tissue of MRSA infection has been successful.
Studies in diabetic patients reported significantly shorter treatment
times than those achieved with standard treatments.
[121][122][123]
Many antibiotics against MRSA are in phase II and phase III clinical trials. e.g.:
Pre-clinical
An entirely different and promising approach is
phage therapy (e.g., at the
Eliava Institute in
Georgia[125]), which in mice had a reported efficacy against up to 95% of tested
Staphylococcus isolates.
[126]
On May 18, 2006, a report in
Nature identified a new antibiotic, called
platensimycin, that had demonstrated successful use against MRSA.
[127][128]
A 2010 study noted significant antimicrobial action of Ulmo 90 and
manuka UMF 25+ honey against several microorganisms, including MRSA. The
investigators noted the superior antimicrobial action of Ulmo 90 honey,
and suggested it be investigated further.
[129]
A separate 2010 study examined the use of medical-grade honey against
several antibiotic-resistant strains of bacteria, including MRSA. The
study concluded that the antimicrobial action of the honey studied was
due to the activity of hydrogen peroxide, methylglyoxal, and a novel
compound named bee defensin-1.
[130]
Ocean-dwelling living sponges produce compounds that may make MRSA more susceptible to antibiotics.
[131]
Some semi-toxic fungi/mushrooms excrete broad spectrum antibiotics, not all of which have been fully identified.
[132]
Cannabinoids (components of
Cannabis sativa), including
cannabidiol (CBD),
cannabinol (CBN),
cannabichromene (CBC),
tetrahydrocannabinol (THC) and
cannabigerol (CBG), show activity against a variety of MRSA strains.
[133]









